“There is nothing either good or bad, but thinking makes it so.”
, William Shakespeare, Hamlet, Act 2 Scene 2, c. 1600
Shakespeare was writing about perception and moral relativism. He was also, without the vocabulary for it, describing a physiological mechanism that science would take 400 years to document precisely.
The thought that labels an event as threatening produces the same bodily response as the event itself. He was right for reasons he could not have known.
What You Will Learn
- Why the body sends more signals to the brain than the brain sends to the body
- How an imagined threat produces real cortisol, real opioids, and real immune suppression
- What motor imagery research reveals about the thought-to-body direction
- A 5-minute experiment that maps the bidirectional loop from both ends
The Direction Nobody Teaches
Most accounts of the thought-body relationship run in one direction: you have a thought, your body responds. That account is incomplete.
The vagus nerve, the primary communication highway between brain and body, carries approximately 80 to 90 percent of its signals from body to brain, not the reverse. The body is sending considerably more information upward than it receives downward.
Antonio Damasio at the University of Southern California proposed this through the somatic marker hypothesis: before conscious deliberation begins on any decision, the body may have already registered a bias. The hypothesis remains debated rather than confirmed. Somatic states (visceral signals, postural data, cardiac rhythms) influence cognition upstream from awareness. The gut signal is not a metaphor. It is data that arrives before the thought does.
William James in 1884 stated the observation in its most provocative form: “We do not tremble because we are afraid. We are afraid because we tremble.” The James-Lange theory argued that physiological state precedes emotional experience, not the reverse. Research by A.D. Craig at the Barrow Neurological Institute confirmed the structural basis: the brain receives continuously updated maps of bodily state via interoceptive pathways, and those maps actively shape cognitive content.
The body is not the output of thought. It is also the input.
The Direction That Surprises People
The downstream direction is where the counterintuitive findings accumulate.
The brain does not reliably distinguish between a real threat and a thought about a threat. When you vividly imagine a threatening scenario, the hypothalamus-pituitary-adrenal (HPA) axis activates and cortisol is released. The physiological stress response is not waiting for confirmation that the threat is real. It is responding to the representation.
Fabrizio Benedetti at the University of Turin documented the positive side of this mechanism through placebo research: placebo analgesia involves measurable endogenous opioid release, not suggestion. When a participant believes they have received a painkiller, the brain releases real opioids. The effect is reversible with naloxone, which blocks opioid receptors. A belief produced neurochemistry. The nocebo operates identically in reverse: negative expectation produces measurable physiological harm, including elevated pain sensitivity and immune suppression, with no active substance involved.
Alvaro Pascual-Leone at Harvard Medical School demonstrated the motor dimension through a piano study that became a reference point in neuroplasticity research. Participants who mentally rehearsed piano scales, without touching a keyboard, produced significant cortical map expansion in motor regions, smaller than the physical practice group, and the two groups converged only after the mental rehearsal group added a brief physical practice session. The imagined movement partially instantiated the movement at the level of neural organization. The thought prepared the body.
Janice Kiecolt-Glaser at Ohio State University extended the evidence into immunology. Across several decades of research, she documented that sustained psychological stress measurably suppresses natural killer cell activity, slows wound healing, and alters cytokine profiles. Thoughts maintained over time restructure immune function. The mechanism is not metaphorical. It is tissue-level biology.
The Loop
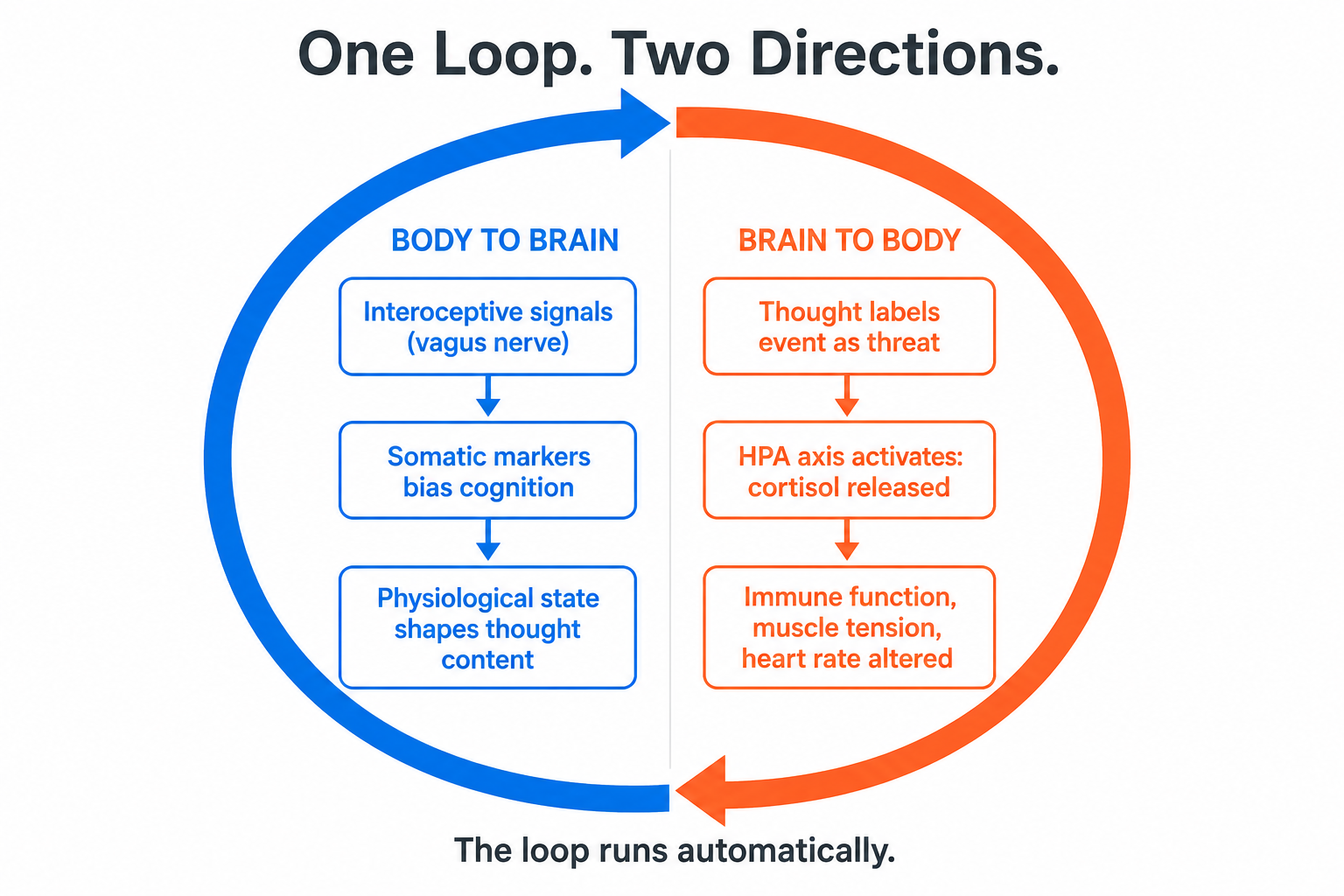
The accurate model is not body-to-thought or thought-to-body. It is a continuous loop running in both directions simultaneously, with each cycle influencing the next.
A physiological state (elevated heart rate, shallow breathing, muscle tension) generates interoceptive signals that the brain interprets as threat-relevant. This primes threat-related thought patterns. Those thought patterns sustain or amplify the physiological state. The loop continues.
Most people never interrupt it because they are not aware they are inside it.
Breathing occupies a structurally unique position here. It is the only autonomic process with a direct voluntary control pathway: the phrenic nerve responds to conscious instruction. Voluntarily changing breath rate and ratio is the fastest accessible entry point into an otherwise automatic bidirectional system.
The 5-Minute Experiment
This maps the loop from both directions. Each part tests one direction of the same mechanism. Neither is a relaxation protocol. Both are measurement tools.
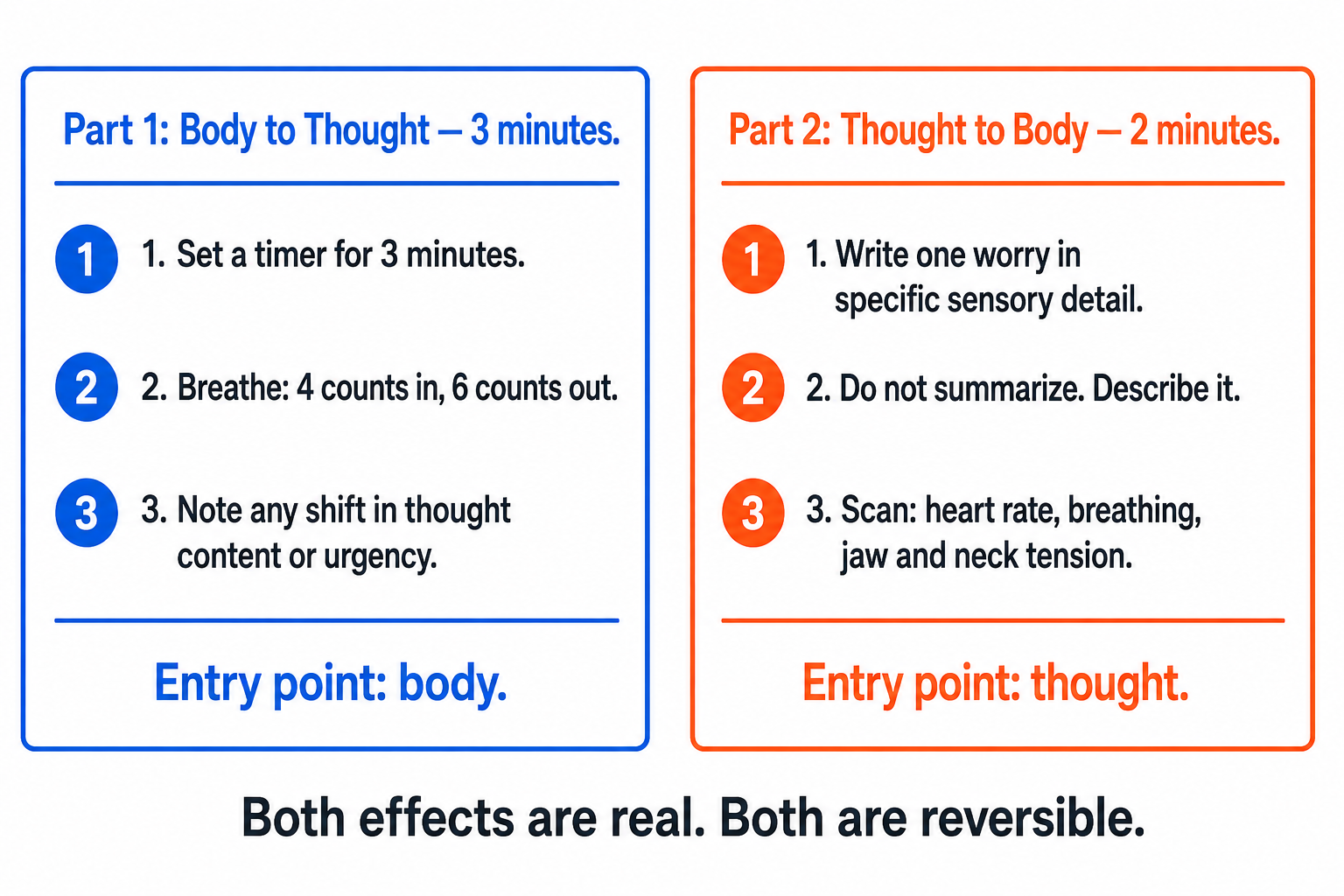
Part 1: Body to thought (3 minutes)
Set a timer for 3 minutes. Breathe at a ratio of 4 counts in, 6 counts out. Keep the exhale consistently longer than the inhale throughout.
Why this ratio: the extended exhale increases cardiac vagal tone via respiratory sinus arrhythmia. As the exhale lengthens, heart rate slows, and the vagus nerve carries that signal upward to the brainstem and on to the locus coeruleus, the brain’s primary norepinephrine-release center. Norepinephrine is the neurochemical most directly associated with threat-appraisal and urgency signaling, and it is plausible, though not firmly established, that its baseline drops as a result. When that happens, the thought content the brain generates tends to shift with it. You are not trying to relax. You are changing the physiological input that shapes what the brain is inclined to think about.
When the timer ends, note two things: whether the content or tone of your thoughts shifted during or after the three minutes, and whether anything that felt urgent before feels less so now. The shift, if it occurs, is the body-to-thought direction of the loop running in real time.
Part 2: Thought to body (2 minutes)
Write down one genuine worry or threat scenario in specific detail. Do not summarize it. Do not write “I am stressed about the project.” Describe the scenario with sensory precision: what the situation looks like, who is in the room, what the specific consequence is, what it would mean.
Why the specificity matters: the brain’s threat-detection circuitry, centered in the amygdala and the hypothalamic-pituitary-adrenal axis, responds to the representational vividness of the scenario, not its factual reality. A vague worry sits below the activation threshold. A detailed, specific mental representation crosses it. Benedetti’s placebo research confirmed this from the positive direction: the more specific and credible the intervention, the larger the neurochemical response. The same logic applies here. You are not catastrophizing. You are testing whether the representation alone, without any external event, is sufficient to produce a measurable physiological change.
After 2 minutes, scan for any of the following: elevated heart rate, changed breathing pattern, muscle tension in the jaw, neck, or shoulders, altered sense of urgency or constriction in the chest.
Both effects are real. Both are reversible. Both confirm the same mechanism from opposite ends.
What This Changes
If the thought-body relationship runs in both directions and forms a continuous loop, then managing cognition is not primarily a cognitive task. It is a physiological one first.
Sleep architecture, movement patterns, breathing mechanics, and nutritional state shape thought quality not because they improve mood, but because they directly determine the prediction inputs the brain is working with. These are upstream variables. Deliberate cognition is downstream from all of them.
Takeaway: A thought is not an event contained in your mind. It is an event in your body. The loop runs whether you are aware of it or not. The only practical question is which direction you choose to enter it from.
The framework for managing the physiological inputs that shape thought begins here: Cultivate Calm: Breath Mastery.
Next in this series: A Feeling Is Not an Emotion. Two words used interchangeably for centuries. Two completely different neural systems.
Sources
Damasio, A. R. (1994). Descartes’ Error: Emotion, Reason and the Human Brain. Penguin Books. [Somatic marker hypothesis]
James, W. (1884). What is an emotion? Mind, 9(34), 188, 205. [James-Lange theory: physiological state precedes emotional experience]
Craig, A. D. (2002). How do you feel? Interoception: the sense of the physiological condition of the body. Nature Reviews Neuroscience, 3(8), 655, 666. [Interoceptive pathways and cognitive influence]
Benedetti, F., et al. (2005). Neurobiological mechanisms of the placebo effect. Journal of Neuroscience, 25(45), 10390, 10402. [Endogenous opioid release and nocebo mechanism]
Pascual-Leone, A., et al. (1995). Modulation of muscle responses evoked by transcranial magnetic stimulation during the acquisition of new fine motor skills. Journal of Neurophysiology, 74(3), 1037, 1045. [Motor imagery and cortical map expansion]
Kiecolt-Glaser, J. K., et al. (2002). Psychoneuroimmunology: Psychological influences on immune function and health. Journal of Consulting and Clinical Psychology, 70(3), 537, 547. [Psychological stress, immune suppression, wound healing]